



Knowing the pathological lesions, sampling and diagnosis of the most common and important swine respiratory conditions, based on the available literature and practical experience is fundamental to address the Porcine Respiratory Disease Complex (PRDC).
![]()

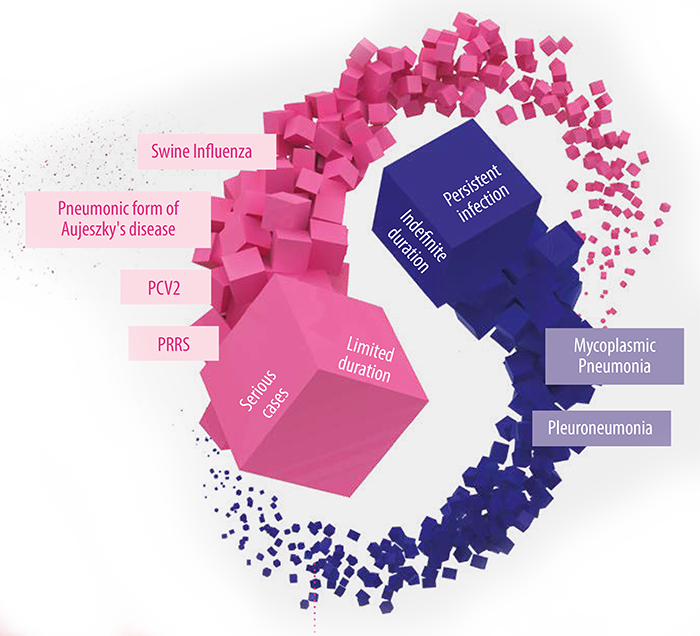
Respiratory diseases in pigs can be classified into two broad categories depending on the extent and duration of the disease:
1.Respiratory diseases that affect a large number of pigs, can be serious and costly, but of limited duration:
![]()

![]()
![]()
![]()
2. Respiratory diseases that persist in a large number of pigs for indefinite periods (Mycoplasmic Pneumonia and Pleuropneumonia).
In these cases, it is difficult to keep the herds free of respiratory diseases, being endemic in many farms.

Respiratory problems in pigs are often the result of multiple agents (co-infection) and rarely due to the effects of a single pathogen, so we usually speak of Porcine Respiratory Disease Complex (PRDC).
Enzootic Pneumonia, for example, when caused only by Mycoplasma is of little relevance. However, when combined with a secondary pathogen such as Pasteurella multocida, the resulting condition can be severe.
First stop
Mastering the necropsy technique
Performing a necropsy is a relatively simple process for which there are different procedures available in the literature. In any case, and independently of the method used, the necropsy should always be ordered, systematic and complete, avoiding leaving important organs or tissues unexamined, regardless of the present symptomatology and the presumptive clinical diagnosis.
To obtain the best performance, the necropsy should be performed as early as possible after the death or sacrifice of the animal. In this article, the authors focus on the opening and examination of the thoracic cavity and respiratory system.
1- Placement of the body
Supine position
Generally, the most common is to use the supine position for young or lactating animals.
To stabilize the body, cuts are made in the axillary region and in the coxofemoral joint, letting the extremities fall under their own weight on the table.
Lateral decubitus
In older or adult pigs, the position in lateral decubitus is more manageable, on the right side, cutting in the axillary and coxofemoral region and dropping the extremities or extracting them to expose the entire thoracic and abdominal wall (Image 1).
Image 1. Stabilization of the body in lateral position.


2- Thoracic cavity opening
Costcondral access
In supine position, two cuts are made on the skin and soft tissues from the mandibular symphysis, forming a triangle to the entrance of the thorax.
Later, a cut is made at the costochondral level on each side to expose the thoracic cavity.
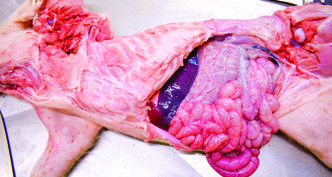
Image 2. Opening of the abdominal cavity in lateral decubitus, with cutting direction from last rib – linea alba – lumbosacral vertebrae.

Costovertebral access
In lateral position, the procedure is easier if the abdominal cavity is opened first:
![]()

![]()
![]()
![]()
![]()
Image 3. Opening of the thoracic cavity in lateral position using the costovertebral junction as support


![]()

3- Extraction of the respiratory system
For a correct and complete examination of the respiratory system, it must be completely removed from the most cranial point.
![]()
![]()
![]()
4- Examination of the respiratory system
For a correct examination of the respiratory system, a longitudinal section is made in the cranio-caudal direction from the larynx to the main bronchi of each lung. This is important to identify possible lesions in the mucosa or abnormal contents in the respiratory tract.
Lung
The examination of the lung should always be done by palpation and includes the evaluation of the following characteristics:
Color: color can give valid information, but often color variations are not diagnostic, especially in animals that have been dead for several hours.
Consistency: changes in lung consistency usually have greater diagnostic value, since they provide information about the presence of edema, areas consolidated by pneumonia, neoplasms, parasitic granulomas, etc.
Sections should be made in the thickness of the different lobes in search of small focal or multifocal intraparenchymal lesions, which may go unnoticed externally or on gross palpation.
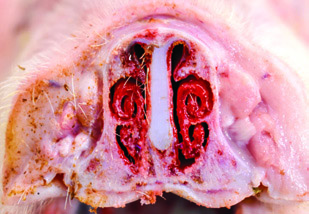
It is important to examine the nasal cavity, especially in cases of chronic or atrophic rhinitis. For this purpose, a cross section of the nasal region is made at the height of the first premolar. This allows us to easily detect alterations in shape or symmetry of the nasal turbinates (Image 4).
Image 4. Opening of the nasal cavity for assessment of the nasal turbinates

(Bibliographic references and further reading recommended are available upon request)